Over 1,200 NObreath® FeNO devices sold since the 2024 UK guideline update.
Bedfont® Scientific Limited, an innovative leader in breath analysis and Fractional exhaled Nitric Oxide (FeNO) testing for asthma care with the NObreath®, welcomes the news that over 1 million people with asthma are now using combination inhalers1 following the joint 2024 asthma guidelines from the National Institute for Care Excellence (NICE), the British Thoracic Society (BTS), and the Scottish Intercollegiate Guidelines Network (SIGN)2. This milestone marks a significant shift in asthma management in the UK, with NObreath® sales exceeding 1,240 units since the update.
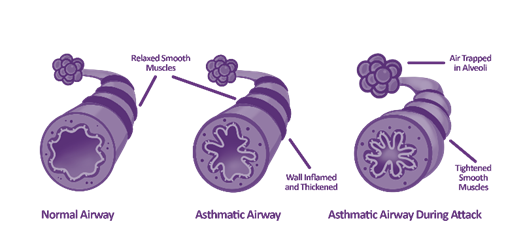
The well-known blue reliever inhaler helps control symptoms but doesn’t address the underlying airway inflammation, the key driver of asthma. Airway inflammation cannot be seen or felt, so whilst patients may not be experiencing any symptoms, the inflammation could be building below the surface, leading to an exacerbation or asthma attack. The NObreath® FeNO device can quickly measure airway inflammation, giving clinicians valuable objective insight enabling them to tailor treatment effectively.
Switching patients to combination inhalers ensures not only symptom relief but also inflammation control. The updated guideline reflects a growing emphasis on prevention-focused asthma care, including earlier anti-inflammatory treatment and reduced reliance on symptom relief alone.
“Seeing more than 1 million people now using combination inhalers marks a significant milestone in the evolution of asthma care. It reflects a growing emphasis on prevention-focused asthma care, including earlier anti-inflammatory treatment and reduced reliance on symptom relief alone. At Bedfont®, we’re proud that FeNO testing is helping support this shift towards more proactive, personalised care. Through the NObreath®, we are helping clinicians gain objective insight into airway inflammation, supporting better-informed decisions and improved long-term outcomes. Everyone deserves access to better asthma care, empowering them to live healthier lives with greater confidence and control.” Said Jason Smith, CEO at Bedfont®.
Bedfont® works closely with its UK distributor, Intermedical UK, to expand access to FeNO testing nationwide. Intermedical launched its NObreath® 3000 campaign last year, signifying a major milestone of 3,000 NObreath® sales in the UK. It also reported growing sales following the guideline update, with over 1,240 devices sold since November 2024 alone, demonstrating the impact of national guidance on asthma care.
A FeNO test with the NObreath® can assess inflammation by measuring nitric oxide (NO) levels in exhaled breath, a biomarker of airway inflammation. The test is quick, easy, and non-invasive, supporting clinicians’ decision-making and treatment plans aligned with evolving guidelines. This milestone reflects a broader shift in asthma care towards precision medicine, biomarker-driven approaches, and more personalised management, all aimed at improving patient outcomes worldwide.
The NObreath® FeNO device has been improving asthma care for over 15 years. To learn more, please visit the website here.
National Institute for Health and Care Excellence. Overview | Asthma: diagnosis, monitoring and chronic asthma management (BTS, NICE, SIGN) | Guidance | NICE [Internet]. Nice.org.uk. NICE; 2024. Available from: https://www.nice.org.uk/guidance/NG245
Asthma is a chronic disease that affects millions worldwide, with many dying from the condition every year1. Asthma care has evolved over the years, but despite the advances, objectively assessing airway inflammation, the key driver of asthma, remains challenging in routine clinical practice.
Historically, asthma management has relied heavily on symptom reporting, but symptoms alone are unreliable indicators of airway inflammation. Inflammation in the airways cannot be seen, and whilst patients may appear clinically stable, airway inflammation may be present, necessitating the use of objective, measurable biomarkers.
FeNO – A non-invasive biomarker technology
Airway inflammation is associated with elevated levels of nitric oxide (NO) in exhaled breath, providing a measurable biomarker of eosinophilic inflammation known as Fractional exhaled Nitric Oxide (FeNO). Using a FeNO device, clinicians can rapidly assess airway inflammation through a non-invasive test that delivers real-time results to support asthma diagnosis, monitoring, and treatment optimisation.
The evolution of FeNO technology
In the 1990s, researchers found that FeNO served as a non-invasive biomarker of airway inflammation and used chemiluminescence technology to measure it, detecting NO through light emitted during a chemical reaction. This method provided high sensitivity and accuracy but proved very costly due to the need for regular maintenance and calibration, limited accessibility, and the specialist training required to operate it. It was clear that early FeNO technology demonstrated clinical value but lacked scalability.
In recent years, this has advanced to electrochemical sensor technology, enabling a new generation of portable FeNO devices, including the NObreath®, whilst still matching the gold-standard chemiluminescence technology.
Modern FeNO devices using electrochemical sensors have decentralised diagnostics, providing a portable respiratory diagnostic option which is easy to integrate into point-of-care workflows. The devices are easy to use and no longer require specialist training, making them a more cost-effective option in respiratory diagnostics.
How point-of-care FeNO testing changes clinical practice
Thanks to continuous innovation, FeNO devices are now accessible at the point of care, enabling faster clinical decision-making, improved monitoring capabilities, and more personalised asthma management. This evolution reflects a broader shift toward decentralised, non-invasive diagnostic technologies designed to support earlier detection and more proactive respiratory care.
FeNO testing – Ease of use
Recent developments in FeNO devices have focused on usability, workflow efficiency, and accessibility. For example, the NObreath®, now in its 2nd generation, is a portable FeNO device which pioneered the exhalation-only manoeuvre. Helping to improve asthma care for over 15 years, the device is suitable for both adults and children, the test is easy to complete and provides a flow incentive to ensure a flow rate of 50 ml/s, yielding an accurate result. Providing instant results, FeNO testing supports efficient point-of-care workflows and faster clinical decision-making.
The future of respiratory diagnostics
The inclusion of FeNO testing in clinical guidelines has increased throughout the years, with the 2024 UK guidance from the National Institute for Health and Care Excellence (NICE), the British Thoracic Society (BTS), and the Scottish Intercollegiate Guidelines Network (SIGN) recommending FeNO as a first-line test to aid asthma diagnosis and management2.
This marks a major shift in asthma care, with a growing emphasis on biomarker-led approaches and more personalised treatment strategies to improve patient outcomes. As respiratory diagnostics become increasingly accessible beyond hospitals and specialist centres, more patients can benefit from advanced technologies through primary care, community clinics, and outpatient respiratory services. Reflecting this trend, Intermedical UK, the exclusive UK distributor of the NObreath® FeNO device, has now installed more than 3,000 devices across the UK, including over 1,200 since the 2024 guideline update, highlighting the rapid adoption of FeNO testing in routine clinical practice.
FeNO testing offers a non-invasive option to aid diagnosis and monitoring of asthma, making biomarker testing more accessible and decentralising respiratory monitoring. Continued innovation in this technology may even expand to home monitoring in the future.
National Institute for Health and Care Excellence. Overview | Asthma: diagnosis, monitoring and chronic asthma management (BTS, NICE, SIGN) | Guidance | NICE [Internet]. Nice.org.uk. NICE; 2024. Available from: https://www.nice.org.uk/guidance/NG245
This article reflects the opinions of a healthcare professional. The views expressed are their own. The intended use for the NObreath® is as follows:
The 2nd generation NObreath® is a breath nitric oxide (NO) test system intended to measure fractional exhaled nitric oxide (FeNO) in parts per billion (ppb) in exhaled breath.
The measurement is taken to evaluate airway inflammation and should be used in conjunction with other clinical and laboratory evaluations where appropriate when making a diagnosis or treatment plan. The measurements are intended for interpretation by healthcare professionals and for us in a healthcare environment, where paediatric and adult patients will complete measurements under supervision.
For many people lungs don’t really feature in their daily self-awareness despite the vital work they do. They are there in the background doing their job. For many people Love your Lungs week might just make them think about what a good job their lungs are doing and maybe look for ways of encouraging them to stay healthy – avoiding pollution, not smoking or vaping and getting regular exercise in for example.
Love Your Lungs Week and Asthma
For those people with asthma Love Your Lungs week might have a different emphasis. Asthma symptoms, whether minor or more dramatic, will certainly make a person aware of their breathing. Good asthma care can help to keep the symptoms under control and avoid bouts of acute symptoms.
Good asthma care starts with an accurate diagnosis. Historically an asthma diagnosis was made on assessment of symptoms, perhaps some lung function testing, and response to treatment. Evidence shows us we sometimes got it wrong using this approach 1. The current joint UK guidelines from British Thoracic Society (BTS), Scottish Intercollegiate Network (SIGN) and National Institute for Health and Care Excellence (NICE)2 have moved to basing a diagnosis of asthma on assessment of symptoms and history that is supported by objective testing. Fractional exhaled nitric oxide (FeNO) is the first recommended test based on clinical accuracy and cost effectiveness. A raised FeNO is an indicator of eosinophilic airway inflammation which is commonly seen in most types of asthma when it is not adequately treated with inhaled corticosteroids (ICS).
Once an accurate diagnosis has been made the person being diagnosed needs to understand what asthma is, what is happening in their lungs, and how their treatment works. There are no agreed education sessions for people newly diagnosed with asthma as there are for those with diabetes.
As asthma is a variable condition, understanding these features support the person to adjust medication to control symptoms and self-manage their condition. Healthcare input is minimal in someone with asthma – an annual review is usually the only planned touch point; others tend to be when the symptoms are poorly controlled. Most healthcare professionals will use a diagram or airway model to explain asthma but the addition of FeNO is a useful tool to demonstrate inflammation especially in the symptomatic person. It helps both practitioner and patient to understand what is happening in the lungs – a measured objective marker demonstrating inflammation.
Why Objective Assessment Remains Important
Many people with a long-term health condition will become so used to the symptoms they experience and the regular use of treatment4. This is seen in some people with asthma – they accept that they have asthma therefore they accept a wheeze or cough4, they stop taking regular ICS treatment and instead rely on a rescue inhaler to treat symptoms as they arise4, or they might continue treatment but fall into bad habits and use their inhaler incorrectly5. In all of these cases measuring FeNO is helpful to assess the underlying airway inflammation, to demonstrate suboptimal control of airway inflammation, and to base ongoing treatment decisions which may require a change of medication, a change of inhaler device or commonly, simply a reminder that asthma treatment needs to be taken regularly with good technique.
The NObreath® FeNO Device
FeNO testing with the NObreath® is a quick and easy non-invasive way to objectively measure airway inflammation. With adult and child test modes, the NObreath® is suitable for all settings thanks to its accuracy and portability. Featuring an exhalation-only manoeuvre, the test is easy to do and can help to improve asthma care, allowing healthcare professionals to tailor asthma treatment effectively.
Love Your Lungs for those with asthma should focus on getting the treatment right and taking it effectively and regularly so that the lungs can get on doing their job without reminding the person they have asthma at all. Of course, that will also include the general measures that everyone else will be considering – avoiding pollution, avoiding smoking and vaping, and getting regular exercise in, but good asthma care will support activity without a symptom burden.
References:
Aaron SD, Vandemheen KL, FitzGerald JM, Ainslie M, Gupta S, Lemière C, Field SK, McIvor RA, Hernandez P, Mayers I, Mulpuru S. Reevaluation of diagnosis in adults with physician-diagnosed asthma. JAMA. 2017;317(3):269-79.
National Institute for Health and Care Excellence. Asthma: diagnosis, monitoring and chronic asthma management (BTS, NICE, SIGN) (NG245) [Internet]. London: NICE; 2024 [cited 2026 18 Jun]. Available from: https://www.nice.org.uk/guidance/ng245
Patel S, Huang M, Miliara S. Understanding treatment adherence in chronic diseases: challenges, consequences, and strategies for improvement. Journal of Clinical Medicine. 2025 Aug;14(17):6034. DOI: 10.3390/jcm14176034.
Canonica GW, Domingo C, Lavoie KL, Kaliasethi A, Khan SQ, Majumdar A, Fulmali S. Asthma patients’ and physicians’ perspectives on the burden and management of asthma: post-hoc analysis of APPaRENT 1 and 2 to assess predictors of treatment adherence. Respiratory medicine. 2024;227:107637.
Bosnic-Anticevich S, Bender BG, Shuler MT, Hess M, Kocks JW. Recognizing and tackling inhaler technique decay in asthma and chronic obstructive pulmonary disesase (COPD) clinical practice. The Journal of Allergy and Clinical Immunology: In Practice. 2023;11(8):2355-64.
Almost 10 months after the National Institute for Health and Care Excellence (NICE), the British Thoracic Society (BTS), and the Scottish Intercollegiate Guidelines Network (SIGN) released an updated joint guideline for asthma care and management, a major milestone has been hit. Over 1 million people are now using combination inhalers instead of relying solely on blue reliever inhalers, marking a major shift towards inflammation-focused asthma management.1
Why does this matter?
Previously, many people living with asthma relied on their blue reliever inhaler, which relieved symptoms, making them feel better quickly. The problem with this was that whilst symptoms were being addressed, the underlying airway inflammation, the main driver of their symptoms, was not being treated. If the inflammation is not treated, symptoms continue to recur, damaging quality of life and increasing over-reliance on medication.1
The problem with symptom-led asthma care.
Patients who rely heavily on Short-Acting Beta-Agonist (SABA) inhalers (rescue inhalers) may report feeling well and believe that their asthma is well controlled because regular use of their inhaler keeps their symptoms at bay.1 When, in reality, this reliance is masking the underlying issue: airway inflammation.
Airway inflammation cannot always be felt, and if left untreated, it could lead to further exacerbations, including asthma attacks.
The shift towards prevention-focused care.2
The update to the guideline placed greater emphasis on treating the underlying inflammation rather than just the symptoms, demonstrating an evolution in asthma care. The updated guidance reflects:
Earlier anti-inflammatory treatment,
Reduced SABA reliance,
Prevention of exacerbations,
More proactive asthma management.
The impact of this guidance is clear: over 1 million people now use combination inhalers to relieve symptoms and treat underlying inflammation, a significant milestone for asthma care.1
Why objective insight matters.
During routine asthma reviews, patients are typically asked about their symptoms, which rely on patient recall. Typically, people with asthma downplay their symptoms, believing that what they experience is typical of their condition.3
And whilst peak flow remains a useful tool in asthma care, it alone may not provide the full picture. It measures airflow obstruction, rather than the inflammatory activity driving asthma, demonstrating the need for objective assessment, because better asthma care starts with better insight.
The role of FeNO testing.2
Fractional exhaled Nitric Oxide (FeNO) testing provides an objective tool to measure airway inflammation. It is non-invasive, easy to do at the point of care and supports:
Diagnosis,
Inhaled corticosteroid (ICS) decisions,
Adherence assessment,
Monitoring,
Evaluation of exacerbation risk.
Aligning with the latest guidance, FeNO supports the move towards more personalised, biomarker-driven asthma care.
The NObreath® FeNO device.
The NObreath® is a modern FeNO device; it is portable and easy to use, making it perfect for primary care. Clinicians can measure a person’s airway inflammation in a short amount of time, fitting perfectly into a standard healthcare appointment. This objective insight enables clinicians to make informed decisions there and then without the need for a follow-up appointment to discuss results.
Combined with an extensive clinical history, a FeNO test with the NObreath® can aid in an asthma diagnosis and tailor treatment appropriately, providing enhanced asthma monitoring.
Precision medicine and the future of asthma care.2
Guidelines are updated as technology and research evolve to improve patient care. The latest guideline from NICE/BTS/SIGN marked a move towards:
Precision medicine,
Biomarkers
Personalised pathways
Earlier intervention,
Better outcomes.
The move towards combination inhalers marks more than a treatment change; it represents a broader evolution in how asthma is understood and managed. Objective insight can provide clinicians with a better understanding of what is going on beneath the surface, with FeNO testing supporting this objective insight and supporting future asthma care.
As asthma care continues to evolve, understanding airway inflammation will become increasingly important in helping clinicians deliver a more personalised and proactive approach.
To learn more about the NObreath® device and how FeNO testing is improving patient outcomes worldwide, visit the website here.
National Institute for Health and Care Excellence. Overview | Asthma: diagnosis, monitoring and chronic asthma management (BTS, NICE, SIGN) | Guidance | NICE [Internet]. Nice.org.uk. NICE; 2024. Available from: https://www.nice.org.uk/guidance/NG245
Bidad N, Barnes N, Griffiths C, Horne R. Understanding patients’ perceptions of asthma control: a qualitative study. European Respiratory Journal. 2018 May 17;51(6):1701346.
The congress, taking place in Istanbul, Türkiye from Friday 12th to Sunday 14th of June, is widely recognised as the world’s largest and most influential meeting dedicated to allergy and clinical immunology. It brings together thousands of clinicians, researchers and healthcare professionals from across the globe each year to share new ideas and showcase innovations in diagnostics, playing a central role in advancing research, education and patient care in allergic diseases such as asthma and food allergy.
“Attending the EAACI Congress 2026 reflects our commitment to strengthening our global network. We look forward to connecting with like-minded organisations, sharing insights into our technology, and exploring new distribution partnerships with those seeking innovative solutions.” Said Jason Smith, CEO at Bedfont®. “We see EAACI as a key opportunity to build relationships that will drive future growth in the allergy and immunology space.”
The Bedfont® team is pleased to be joined by its Turkish distributor, Teknikel, to demonstrate its Fractional exhaled Nitric Oxide (FeNO) and hydrogen and methane breath testing (HMBT) technologies, highlighting how these innovative tools can support improved diagnosis, monitoring, and the management of respiratory and gastrointestinal conditions.
The team will be at stand I03, where you can find the NObreath® FeNO device, which has been improving asthma care and management for over 15 years, providing an objective insight into airway inflammation, a key driver of asthma symptoms. And the Gastrolyzer® range of HMBT devices, which have been aiding gastrointestinal investigation for over 35 years, enabling clinicians to tailor treatment effectively.
For Bedfont®, this congress is invaluable not only for showcasing its solutions but also for engaging with partners and stakeholders as it continues to advance technology and expand its global reach. To learn more, visit the website here.
Bedfont® Scientific Limited to showcase why the NObreath® is the FeNO device of choice at this year’s global event.
World leaders in breath analysis Bedfont® Scientific Ltd. are pleased to be attending this years American Thoracic Society (ATS) International Conference, to exhibit the innovative NObreath® Fractional exhaled Nitric Oxide (FeNO) device at booth 1236 alongside its US distributor coVita™. Bedfont® is an innovative MedTech company with nearly 50 years of expertise in the design and manufacture of medical breath analysis devices, helping to improve patient outcomes worldwide.
The ATS International Conference, taking place from the 15th and 20th May at the Orange County Convention Centre in Orlando, Florida, is a global event attracting more than 15,000 experts in pulmonary, critical care and sleep medicine to share groundbreaking research and advance clinical practice. Bedfont® will be sharing how the NObreath® is revolutionising asthma care worldwide.
The team can be found at booth 1236, where they will showcase the NObreath®, which has been helping to improve asthma care and management for over 15 years by providing objective insight into airway inflammation, a key feature of asthma. It enables clinicians to measure inflammation non-invasively, supporting a future where today’s science meets tomorrow’s care.
“We’re excited to be part of ATS this year and to bring our expert team together on the stand to engage with the global respiratory community. We invite attendees to come and speak with us, experience our technology firsthand, and explore how we can work together.” Said Jason Smith, CEO at Bedfont®. “ATS provides an important platform for us to showcase the NObreath® and its impact in respiratory care.”
Joining Bedfont® and coVita™ at booth 1236 is Medical Advisory Board Member, Carol Stonham MBE, a respiratory expert who serves as the Children and Young People Asthma Clinical Lead at Gloucestershire ICB. Carol will be bringing a wealth of knowledge to the event and will be hosting a talk at Innovation Hub 3 on Sunday 17th May at 1:15 pm EDT; where she will explore the role of FeNO in practice and discuss emerging opportunities.
You will find the Bedfont® team at booth 1236 between the 17th and 19th May, to find out more visit the website here.
In 2019, 262 million people worldwide had asthma, with 455,000 deaths from the chronic condition1, stark figures that highlight asthma control still needs improvement. Most people living with asthma believe that no physical symptoms mean their asthma is controlled, but this is sadly not always the case. Airway inflammation is the underlying cause of asthma, something that cannot be seen and not always felt.
Many asthma patients feel fine until they don’t. Objectively measuring airway inflammation with Fractional exhaled Nitric Oxide (FeNO) testing is a vital way to prevent exacerbations and improve overall asthma care.
What is FeNO and why does it matter2?
When airways are inflamed, they produce excess nitric oxide (NO), a gas that can be measured by performing a FeNO test. A FeNO test provides insight into a person’s airway inflammation by measuring NO levels in exhaled breath.
High FeNO levels indicate eosinophilic airway inflammation. The higher the reading, the more severe the inflammation is.
By measuring airway inflammation, healthcare professionals can use the results to aid an asthma diagnosis and tailor treatment appropriately.
Limitations of traditional asthma monitoring.
Traditionally, clinicians have relied on patients relaying their symptoms, which doesn’t always give the full picture of a person’s asthma. Many people believe that because they have asthma, they should have a cough and they should have a wheeze, and they downplay their symptoms.
Providing a FeNO test at regular asthma reviews empowers healthcare professionals to detect airway inflammation early, allowing them to monitor medication response and personalise treatment. This ultimately can catch an exacerbation early and get patients back on track with well-controlled asthma.
Additionally, medication adherence rates range from 30% to 70%3. A patient may report taking their medication regularly and using the correct technique; however, a quick, easy FeNO test can reveal poor adherence. Showing a patient their airway inflammation can create an opportunity to discuss and reinforce the importance of good adherence and technique.
Recent advancements in FeNO testing.
In the 1990s, researchers found that FeNO served as a non-invasive biomarker of airway inflammation and used chemiluminescence to measure it. This method proved very costly due to regular maintenance and calibration, and difficult to access because of the machines’ size and the specialist training required.
In recent years, this has advanced to electrochemical sensor technology, enabling more cost-effective, portable FeNO devices like the NObreath®, whilst still matching the gold-standard technology of chemiluminescence. Thanks to continuous innovation, FeNO devices are now accessible at the point of care and provide instant results, improving patient outcomes.
To learn more about chemiluminescence and electrochemical sensor technology, read our article here.
In the late 1990s, FeNO began to appear in international clinical practice guidelines for asthma, and the American Thoracic Society (ATS) officially recommended its use to assess airway inflammation in adults and children in 20114.
Since then, FeNO testing has been recommended in asthma guidelines across the world, with the most recent joint guidance from the National Institute for Health and Care Excellence (NICE), the British Thoracic Society (BTS), and the Scottish Intercollegiate Guidelines Network (SIGN), recommending FeNO as a first-line test for asthma diagnosis5.
To learn more about the global guidelines on asthma care and management, read our article here.
The NObreath® FeNO device
The NObreath® was developed in 2008, designed with healthcare professionals and patients in mind. It provides a non-invasive, fairly priced option for FeNO testing, making it more accessible to healthcare providers worldwide.
Featuring an adult and child test mode, the NObreath® is suitable for all settings thanks to its accuracy and portability. It requires an exhalation-only manoeuvre, making it a quick and easy test to take for both adults and children.
The device was designed with the patient in mind and features multiple flow incentive screens. These incentive screens not only engage the patient, but they also ensure a correct flow rate of 50 ml/s, providing an accurate test result.
To learn more about FeNO testing with the NObreath®, visit the website here.
Many deaths from asthma are thought to be preventable, meaning better asthma care is needed. Advances in FeNO testing have been instrumental in improving asthma control, and with increasing recognition in global asthma guidelines, FeNO testing can make a difference.
To learn more about Bedfont® Scientific Limited, world leaders in breath analysis with over 49 years of expertise in the medical device industry, visit the website here.
Dweik RA, Boggs PB, Erzurum SC, Irvin CG, Leigh MW, Lundberg JO, et al. An official ATS clinical practice guideline: interpretation of exhaled nitric oxide levels (FENO) for clinical applications. American journal of respiratory and critical care medicine [Internet]. 2011;184(5):602–15. Available from: https://www.ncbi.nlm.nih.gov/pubmed/21885636/
National Institute for Health and Care Excellence. Overview | Asthma: diagnosis, monitoring and chronic asthma management (BTS, NICE, SIGN) | Guidance | NICE [Internet]. Nice.org.uk. NICE; 2024. Available from: https://www.nice.org.uk/guidance/NG245
Over 28 million people in the United States (US) have asthma1,2, with the condition named as the leading chronic disease in children, affecting approximately 4.9 million under the age of 182,3. In the US, asthma is one of the most common and costly diseases, and these stark figures highlight why asthma still matters, even in 2026. This Asthma and Allergy Awareness Month, we are exploring the prevalence of asthma and how advancing technology can make a difference.
Asthma places a significant burden on healthcare and the economy, with annual economic costs between 2008 and 2013 contributing to:
$3 billion in losses due to missed work and school days,
$29 billion due to asthma-related mortality,
$50.3 billion in medical costs.
The numbers prove that asthma is common, but it is important to remember that this chronic condition is also manageable; however, outcomes are not equal, and certain populations are disproportionately affected. These disparities are shaped by a combination of structural, social, biological, and behavioural factors. Structural inequities, such as5:
Systemic racism,
Residential segregation,
Discriminatory policies,
Often influence the conditions in which people live, work, and access care. These, in turn, affect social determinants like income, education, housing quality, environmental exposures, and access to healthcare. While biological factors such as genetics and individual behaviours like smoking or medication adherence play a role, it is these broader social and structural inequities that largely drive unequal asthma outcomes across populations.
The hidden problem: Poor asthma control
Millions of people are diagnosed with asthma, with many of them not having the condition well managed. It is estimated that 44% of children with asthma have uncontrolled asthma6, which can lead to exacerbations and severe asthma attacks.
Many asthma patients rely heavily on rescue inhalers, which relieve the immediate symptoms but do not address the underlying airway inflammation. This quick relief can make patients feel in control of their asthma, but without addressing the root cause, asthma remains uncontrolled beneath the surface.
Another contributor to poorly controlled asthma is misdiagnosis. Asthma is not a single condition; it can be allergic/eosinophilic or non-eosinophilic. If the asthma is not diagnosed correctly, this can lead to ineffective or over/under treatment. If the underlying asthma type isn’t properly diagnosed, the treatment cannot be matched to the disease type.
Additionally, a lack of objective measurement in routine care can affect asthma control. Traditionally, asthma management has relied on:
Symptoms,
Patient recall,
Peak flow.
The problem with just focusing on these points is that clinicians may over- or underestimate control, which leads to escalating or reducing treatment inappropriately. Symptoms do not always reflect underlying inflammation and may lead to missed opportunities for early intervention.
This is where better access to objective, point-of-care tools, such as Fractional exhaled Nitric Oxide (FeNO) testing, is needed. Without objective measurement, asthma care often relies on what can be seen and heard, not on what’s happening at the inflammatory level inside.
What is FeNO testing7?
A FeNO test is a quick, easy, non-invasive way to measure airway inflammation, specifically eosinophilic inflammation. When airways are inflamed, higher levels of nitric oxide (NO) are produced. This gas can be detected in exhaled breath, with higher levels indicating inflammation, making FeNO testing a vital tool for asthma care and management.
With FeNO providing a non-invasive, quick point-of-care test, it can help identify type 2 inflammation and predict steroid responsiveness, helping clinicians see inflammation that symptoms alone cannot reveal.
How FeNO improves decision-making
FeNO fits into the whole asthma pathway; it’s not just a diagnostic tool; it can also help treat and manage asthma. Diagnosing and managing this chronic condition isn’t always straightforward, and in the past, healthcare professionals have relied on guesswork. FeNO testing changes that, it can:
Support a diagnosis of asthma,
Guide inhaled corticosteroid (ICS) use,
Monitor medication adherence,
Predict exacerbation risk,
Reduce unnecessary medication escalation.
FeNO is recognised in global guidelines for asthma care and management, with the ATS/ERS guidance positioning FeNO as a practical tool to support diagnosis, guide anti-inflammatory treatment, and monitor airway inflammation, helping clinicians move from symptom-based to more objective asthma care8.
Expanding access to FeNO testing
Objective testing has the potential to transform asthma care, but access remains a challenge. Limited availability outside specialist centres, time constraints in primary care, and geographic inequalities have all contributed to the underuse of tools such as FeNO. The result is a gap between what is possible and what is delivered in everyday care. Advances in technology only matter if people can access them.
Bedfont® Scientific Limited, an innovative MedTech company based in the UK with nearly 50 years of experience in medical breath analysis, has been improving asthma care and management worldwide for over 15 years with its NObreath® FeNO device. Working closely with its US distributor, coVita™, it has been working hard to improve access to FeNO testing by providing a fairly priced, low-maintenance FeNO device.
In 2025, the NObreath® became the allergists’ FeNO device of choice in the US, with Allergy Partners offering FeNO testing with the NObreath® through more than 125 locations in over 20 states. This partnership ensures that FeNO testing is being integrated into routine care, not just specialist settings, allowing more patients to get tested closer to home.
The future of asthma care
This Asthma and Allergy Awareness Month, we want to focus on how early intervention can lead to better long-term outcomes for asthma patients. Advances in technology mean that objective testing, such as FeNO, is more widely accessible, which is vital as biomarker-driven care becomes the standard. FeNO devices like the NObreath® provide clinicians with more insight into underlying inflammation that cannot be seen, enabling improved patient care.
To learn more about the NObreath® FeNO device and how it is improving precision in asthma care, visit the website here.
References
NCHS/DHIS. NHIS Adult Summary Health Statistics [Internet]. Cdc.gov. 2021. Available from: https://data.cdc.gov/National-Center-for-Health-Statistics/NHIS-Adult-Summary-Health-Statistics/25m4-6qqq/about_data
NCHS/DHIS. NHIS Child Summary Health Statistics [Internet]. Cdc.gov. 2021. Available from: https://data.cdc.gov/National-Center-for-Health-Statistics/NHIS-Child-Summary-Health-Statistics/wxz7-ekz9/about_data
Ferrante G, La Grutta S. The Burden of Pediatric Asthma. Frontiers in Pediatrics [Internet]. 2018 Jun 22;6(186):1–7. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6023992/
Nurmagambetov T, Kuwahara R, Garbe P. The Economic Burden of Asthma in the United States, 2008–2013. Annals of the American Thoracic Society [Internet]. 2018 Mar;15(3):348–56. Available from: https://pubmed.ncbi.nlm.nih.gov/29323930/
Asthma and Allergy Foundation of America. Asthma Disparities in America [Internet]. Asthma & Allergy Foundation of America. 2020. Available from: https://aafa.org/asthma-allergy-research/our-research/asthma-disparities-burden-on-minorities/
CDC Archives [Internet]. archive.cdc.gov. Available from: https://archive.cdc.gov/#/details?url=https://www.cdc.gov/asthma/asthma_stats/uncontrolled-asthma-children-2018-2020.htm
What is a FeNO Test? [Internet]. Aaaai.org. 2021. Available from: https://www.aaaai.org/Tools-for-the-Public/Conditions-Library/Asthma/What-Is-A-FeNO-Test
Murphy RC, Zhang P, Tejwani V, Khatri SB, Hallstrand TS, Ruminjo JK, et al. Summary for Clinicians: Clinical Practice Guideline for the Use of Fractional Exhaled Nitric Oxide to Guide the Treatment of Asthma. Annals of the American Thoracic Society. 2022 Oct;19(10):1627–30.
The NObreath® FeNO device offers a clear pathway to more effective asthma care, reducing over-reliance on blue inhalers.
Bedfont® Scientific Limited, an innovative med-tech company specialising in medical breath analysis devices, welcomes the new study at University Hospital Southampton exploring whether enhanced asthma check-ups can reduce inhaler use among children. For over 15 years, Bedfont® has supported improved asthma care with its NObreath® Fractional exhaled Nitric Oxide (FeNO) device, which measures airway inflammation through exhaled breath. The quick and easy test provides clinicians with objective insight to guide medication decisions, reduce unnecessary reliever prescriptions, prevent over-reliance on blue inhalers, and help avoid future asthma attacks.
Research has found that children using 6 or more blue reliever inhalers a year are 3-5 times more likely to have an asthma attack1. Reliever inhalers only treat the immediate symptoms and mask the underlying airway inflammation, which can lead to further exacerbations.
The study aims to create a new alert system that automatically notifies general practitioners (GPs) when a child has been prescribed too many inhalers, prompting an immediate check-up. This will allow healthcare professionals to perform a review and help prevent future attacks.
Jason Smith, CEO at Bedfont®, comments, “We welcome the focus this important study brings to the growing problem of reliever inhaler over-use in children, a clear signal that many young people are still not getting the right support for long-term asthma control. Over-reliance on blue inhalers often reflects unmanaged airway inflammation and missed opportunities for targeted treatment. That’s why we continue to advocate for improving the accessibility of FeNO testing in primary care, a guideline-recommended, evidence-based tool that helps clinicians identify and treat underlying inflammation early. With better access to FeNO testing across the UK, we can help reduce unnecessary reliever use, improve outcomes for children, and support GPs in delivering truly personalised asthma care.”
Although FeNO testing is now recommended as a first-line test in UK asthma guidelines, access remains inconsistent across primary care. As a result, many children continue to be managed without the benefit of objective airway inflammation testing, increasing the risk of poorly controlled asthma and over-reliance on reliever inhalers. Reliever inhaler overuse in children is a well-recognised marker of uncontrolled asthma and is associated with a higher risk of exacerbations and emergency admissions.
Greater investment and targeted funding are urgently needed to support the widespread adoption of FeNO technology in primary care, helping clinicians deliver earlier, more accurate diagnoses and reduce preventable harm. To learn more about the NObreath® and how it can help asthma care and management, visit the website here.
References
News I. Southampton researchers lead UK-first study to target “dangerous” asthma inhaler overuse [Internet]. ITV News. 2026 [cited 2026 Mar 3]. Available from: https://www.itv.com/news/meridian/2026-02-25/uk-first-study-targets-dangerous-overuse-of-asthma-inhalers-in-children
Asthma is a chronic lung condition that causes airway inflammation and affects approximately 262 million people worldwide1. Typical symptoms include:
Wheezing,
Breathlessness,
Chest tightness,
Coughing.
When airways are inflamed, breathing can become difficult. Recent Asthma + Lung UK research found that over 42,000 people ended up in emergency care in 2023/24 after visiting 5 or more times within the last 12 months2. These startling numbers highlight the importance of better asthma management to reduce the burden on healthcare systems.
Assessing airway inflammation is key to better asthma management. When a person’s airways become inflamed, higher-than-usual nitric oxide (NO) gases are produced. The easiest way to measure a person’s NO levels is a Fractional exhaled Nitric Oxide (FeNO) test.
What is FeNO testing?
A FeNO test with a device like the NObreath® is a quick, easy, non-invasive and accurate way to measure NO levels in exhaled breath. NO is a marker of eosinophilic airway inflammation, common in allergic asthma. Patients follow on-screen instructions to inhale and then exhale into the device, providing instant results.
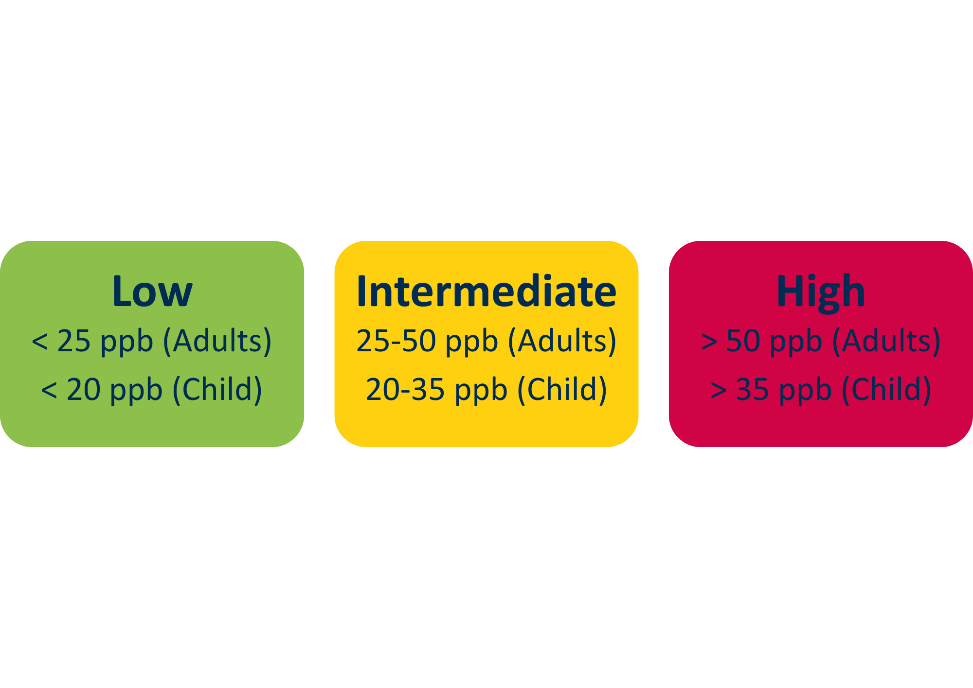
FeNO levels are measured in parts per billion (ppb). A high FeNO level indicates airway inflammation and can aid in diagnosing asthma.
ATS/ERS Clinical Guidelines Summary for Interpreting FeNO Levels3,4:
Note: These reflect the ATS and ERS guidelines. FeNO interpretation thresholds may vary between guidelines.
FeNO testing with the NObreath®
The NObreath® is a FeNO device manufactured by Bedfont® Scientific Limited. Bedfont® has over 48 years of knowledge and expertise in designing and manufacturing medical breath analysis devices. The NObreath® has improved asthma management for over 15 years, providing healthcare professionals (HCPs) with a fairly priced solution for FeNO testing. Suitable for both adults and children, the NObreath® is perfect for primary and secondary care settings. For more information on the NObreath®, visit the website here.
Why is FeNO testing useful in asthma?
Airway inflammation cannot be seen; FeNO tests allow HCPs to track any underlying inflammation and, when used alongside an extensive clinical history, can diagnose asthma. Having access to a FeNO device is useful throughout the asthma pathway. Not only does it aid an asthma diagnosis, but it also helps to guide treatment decisions.
Carrying out FeNO tests in routine asthma reviews allows HCPs to:
Tailor inhaled corticosteroid (ICS) therapy,
Identify steroid responsiveness,
Guide step-up or step-down treatment strategies.
A patient who consistently presents with a high FeNO level indicates possible poor adherence to ICS, therefore, instigating conversations about medication use.
FeNO testing is incorporated into worldwide guidelines. Joint guidelines by the National Institute of Health Excellence (NICE), the British Thoracic Society (BTS), and the Scottish Intercollegiate Guidelines Network (SIGN) now recommend FeNO as a first-line test for asthma diagnosis.
Future of FeNO testing.
The biggest challenge with FeNO testing is accessibility; unfortunately, some areas do not have access to a FeNO device. In a recent interview with Carol Stonham MBE, we discussed the issues around funding. In some areas, the Integrated Care Board (ICB) will pay for it, but in others, it is down to the Primary Care Network (PCN). However, if the PCN does not deem it a priority, it comes down to the individual General Practice (GP) surgeries.
Looking back at the shocking statistics at the beginning of this blog, it is clear that better asthma management is needed. FeNO is a valuable tool in modern asthma management. It guides HCPs to understand the underlying airway inflammation in asthma, leading to better patient outcomes.
With the NICE/BTS/SIGN guidelines update, FeNO testing is recommended as a first-line test for asthma diagnosis and management in adults. This means access to FeNO needs to improve.
For more information on FeNO testing and its central role in asthma care in the joint NICE/BTS/SIGN guidelines, click here to read our article on the guideline updates and FeNO testing.
Louis R, Satia I, Ojanguren I, Schleich F, Bonini M, Tonia T, Rigau D, Ten Brinke A, Buhl R, Loukides S, Kocks JW. European Respiratory Society guidelines for the diagnosis of asthma in adults. European Respiratory Journal. 2022 Sep 1;60(3). DOI: 10.1183/13993003.01585-202. [cited 2025 May 14] Available from: https://pubmed.ncbi.nlm.nih.gov/35169025/
Dweik RA, Boggs PB, Erzurum SC, Irvin CG, Leigh MW, Lundberg JO, Olin AC, Plummer AL, Taylor DR, American Thoracic Society Committee on Interpretation of Exhaled Nitric Oxide Levels (FENO) for Clinical Applications. An official ATS clinical practice guideline: interpretation of exhaled nitric oxide levels (FENO) for clinical applications. American journal of respiratory and critical care medicine. 2011 Sep 1;184(5):602-15. PMCID: PMC4408724 PMID: 21885636. [cited 2025 May 14] Available from: https://pubmed.ncbi.nlm.nih.gov/21885636/