With the festive holiday season upon us, many tend to indulge in the various rich, festive treats on offer. December is a joyful time; it is also a time to relax and treat yourself; however, the festive eating can take its toll on digestive health. A recent survey by King Edward VII’s Hospital found that 6 in 10 people blame their festive digestive issues on overindulgence1. In this blog, we will explore how HMBT can help you take a closer look at your gut health and identify any underlying conditions that may be causing your discomfort.
Common holiday eating habits and their impact
Typically, in December, we have a higher intake of sugar, fat, and alcohol. This is due to the tasty treats on offer and the extra socialising during this period. Some view the festivities as a time to relax from their regular eating habits and find themselves eating at irregular times. In contrast, others find the festive period a particularly stressful time, which can result in stress eating. As the gut microbiome can be very sensitive to dietary changes, you may find you suffer from bloating, gas, reflux, and irregular bowel movements during the festive period.
What is HMBT?
Hydrogen-methane breath testing is a non-invasive method for measuring hydrogen (H2) and methane (CH4) gases in exhaled breath. Gut bacteria produce these gases during the fermentation of undigested carbohydrates, and high levels of these gases can indicate an underlying issue. A HMBT can help identify gastrointestinal disorders like:
Small Intestinal Bacterial Overgrowth (SIBO).
Fructose/lactose intolerance.
General fermentation imbalances.
HMBT with the Gastrolyzer® range
The Gastrolyzer® is a range of HMBT devices used to aid in gastrointestinal investigation. A test using the Gastro+™ and GastroCH4ECK® is a simple, non-invasive method for measuring hydrogen and methane gases in exhaled breath. The Gastro+™ is a hand-held portable hydrogen device for quick and easy breath analysis, and the GastroCH4ECK® is a breath hydrogen and methane device with direct breath testing, allowing you to take a reading there and then, with instant results. The GastroCH4ECK® also allows for remote breath testing, allowing patients to undergo a HMBT in the comfort of their own homes.
How HMBT can help after the holidays
If you experience gastrointestinal issues, it is essential to consult a healthcare professional for evaluation. Some individuals may find that their issues resolve once they return to their normal routine; however, a HMBT can help identify sugar intolerance, such as lactose intolerance, which can help guide you in respect to what you eat during the festive period. Hydrogen-methane breath testing can also be used to support tailored dietary plans aimed at restoring gut health after the holidays.
December is a time for joy and indulgence, but balance is key. Try to avoid overindulging excessively, and ensure your diet during this period includes fibre, prebiotics, and probiotics. It is also vital to stay hydrated. By incorporating these into your festive diet, you can help minimise gastrointestinal discomfort, leaving you free to enjoy the holidays without the discomfort.
To learn more about HMBT and the Gastrolyzer® range, please visit our website here.
Rbeck Healthtech Private completes registration for the NObreath® FeNO device, helping to improve asthma care across the region.
Bedfont® Scientific Limited, world leaders in breath analysis, with over 48 years of experience in designing and manufacturing medical breath analysis devices, has collaborated with Rbeck Healtech Private to make Fractional exhaled Nitric Oxide (FeNO) testing more accessible in India. Rbeck Healthtech Private is an entirely diverse healthcare equipment distributor, with a portfolio specialising in pulmonology, cardiology, and rehabilitation. It has recently added the innovative NObreath® device to its offerings, expanding access to FeNO testing in India.
Asthma is a chronic lung disease which cannot be cured; however, with the correct diagnosis and treatment, people with asthma can lead normal lives. India accounts for approximately 13.1% of the global asthma burden1, meaning that improving access to essential diagnostic and management tools, such as the NObreath®, is vital. The NObreath® measures FeNO levels on exhaled breath, a key indicator in type 2 airway inflammation, which is commonly found in asthma.
Jason Smith, CEO at Bedfont®, comments, “Partnering with Rbeck Healthtech and the successful registration for the NObreath® in India is a meaningful milestone in our mission to make precision asthma care accessible worldwide. India faces a significant burden of asthma, and we believe that FeNO testing can empower clinicians with clearer insights into airway inflammation, leading to more personalised and effective treatment decisions.”
With the Global Asthma Report 2022 indicating that a considerable proportion of asthmatic individuals remain underdiagnosed or untreated2 in India, it is hoped that this strategic partnership will help expand the accessibility of FeNO testing in the region, ultimately saving lives.
To find out more about the NObreath® and how it is improving asthma care worldwide, visit the website here.
References
1.Singh S, Salvi S, Mangal DK, Singh M, Awasthi S, Mahesh PA, et al. Prevalence, time trends and treatment practices of asthma in India: the Global Asthma Network study. ERJ Open Research [Internet]. 2022 May 30;8(2):00528-2021. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9149387/
Part 3: Asthma treatment in 2024: Navigating the new recommendations for every age
After exploring diagnostic changes and the pivotal role of Fractional exhaled Nitric Oxide (FeNO) in asthma care, part 3 of our series shifts the focus to treatment and long-term management. From the latest recommendations for patients aged 12 and over, as well as tailored treatment pathways for children under 5, this blog summarises practical, guideline-driven approaches for managing asthma more effectively.
Treatment for patients ages 12 and over
In the past, patients with asthma have always been told to carry their blue inhaler, as this will keep them safe in the event of an asthma attack. This is no longer the case in the new guidelines.
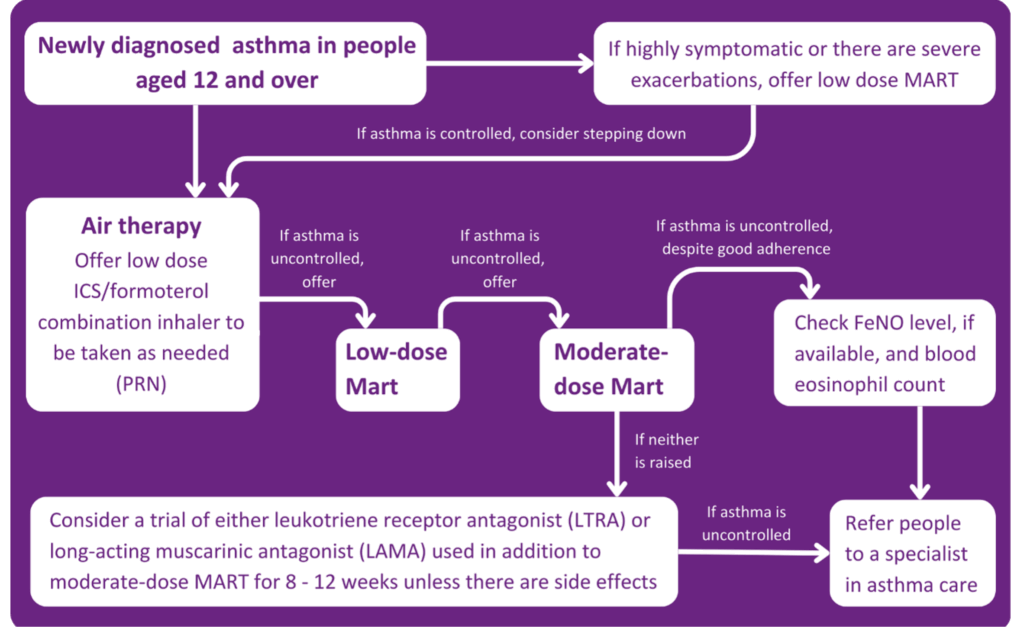
It is now recommended that people aged 12 and above with a new diagnosis of asthma should be offered Anti-Inflammatory Relief (AIR) therapy. This means using a formoterol-containing inhaled steroid inhaler on an as-needed basis. This process is for someone not experiencing symptoms at the time of presentation.
If a patient is unwell or exacerbating, this step should be skipped, and the patient should be offered low-dose Maintenance and Reliever Therapy (MART). MART is an asthma treatment plan in which one combination inhaler is used instead of two separate preventer and reliever inhalers.
If a patient is still symptomatic after being on a low-dose MART regime, then a moderate-dose MART regime should be offered. If this doesn’t relieve symptoms, inhaler technique, adherence, and new triggers should be assessed.
At this point, if a person is still symptomatic, it is important to understand what is causing the symptoms. Is it uncontrolled eosinophilic airway inflammation, or is it that the inflammation is controlled and it is bronchospasm? A FeNO test will measure the patient’s FeNO level. If it is raised, a referral to an asthma care specialist is required. If the FeNO level isn’t raised, the patient should be offered either a Leukotriene Receptor Antagonist (LTRA) or a Long-Acting Muscarinic Antagonist (LAMA) on top of a moderate-dose MART regimen for 8-12 weeks.
If at the end of the 8-12 weeks:
The asthma is controlled, continue with the treatment.
If this control has improved but still not completely, continue the treatment or add the LTRA or LAMA (Whichever is not already being taken).
If the control hasn’t improved, stop the LTRA or LAMA being taken and replace it with the alternative.
If, after these steps, the asthma remains uncontrolled, the patient should be referred to a specialist.
For patients with an existing asthma diagnosis and currently on treatment recommended in the previous guideline, nothing needs to change as long as the asthma is controlled and not much salbutamol is being used. If, however, the patient is only using salbutamol with no other inhalers, it should be considered to push them over to an AIR regime.
If patients on a low-dose inhaled steroid and not using a MART regimen become symptomatic, they should be moved to a low-dose MART regimen, and if on a moderate-dose steroid, then to a moderate-dose MART regimen.
If the patient is still experiencing symptoms after this, they should be referred to a specialist. If you have patients on a high-dose steroid and they are symptomatic, they should also be referred.
The guidelines also state that before any medication is adjusted or changed, you must address the possible reasons why the asthma is uncontrolled. For example:
Currently, no inhalers are licenced for MART in children, even though the guidelines include MART for consideration in treatment. Just because the licensing isn’t available now doesn’t mean MART cannot be used for children; it can be prescribed off-label. In this case, it should be documented that medication is being used off-label under the current guidelines by NICE/BTS/SIGN 2024.
Previously, the Quality and Outcomes Framework (QOF) said spirometry and one other test should be conducted; however, that has now changed in line with the current guidance. You should now look at the number of patients newly diagnosed with asthma who have had one of the following tests:
Eosinophil count,
FeNO,
Spirometry,
Peak flow with Bronchodilator Response (BDR),
Bronchial responsiveness (In adults),
Skin prick test or blood IgE (In children).
This is between 3 months before or 3 months after diagnosis. The diagnosis must be coded correctly to qualify for QOF points.
Monitoring asthma
At every asthma review, asthma control should be monitored by asking the following questions:
Has there been any absence from work or school due to asthma?
How much reliever inhaler is being used, including a check of the prescription record.
The number of courses of oral corticosteroids.
Have there been any hospital admissions or emergency visits due to asthma?
The guidelines recommend using an asthma control test at reviews and say not to use peak flow to assess asthma control unless there is a person-specific reason to do so. FeNO testing should also be considered in reviews for adults and before and after changing asthma medication.
Poor asthma control
If a patient has poor asthma control, it is recommended to check their FeNO level, as this may indicate poor adherence to treatment or the need for an increased dose of Inhaled Corticosteroids (ICS).
A Short-Acting Beta2 Agonist (SABA) should no longer be prescribed without an ICS, and if any change to asthma medication is made, you should review the response within 8-12 weeks.
Changing medication
There is now also guidance on what you should base the choice of inhalers on. The following must be considered:
Can the patient use the inhaler correctly?
The patient’s preference for inhalers.
The lowest environmental impact among suitable devices.
The presence of a dose counter.
It is also noted that a spacer should be prescribed with a metered dose inhaler, particularly in children.
The inhaler technique must be checked at every asthma review when control deteriorates and if the inhaler changes. A suitable alternative should be found if the patient cannot use the device correctly.
Risk care
HCPs should consider identifying asthma patients who are more at risk of poor outcomes. Risk factors to consider are:
Non-adherence to medication.
Overuse of SABA inhalers (More than two a year).
Needing two or more courses of corticosteroids per year.
Two or more emergency or hospital admissions for asthma per year.
This is just a recommendation to evaluate those who are more at risk; you should not forget about the other patients.
The latest guidelines from NICE, BTS, and SIGN introduce significant changes to the diagnosis and management of asthma. While adapting to these updates may initially be challenging, proper education and resources will help healthcare professionals integrate them effectively. In the long run, this unified approach will enhance asthma care for thousands of patients and improve outcomes.
To watch the full webinar, ‘Practical Insights for Asthma Care. The New NICE/BTS/SIGN Guidelines. Why FeNO First?’, click here.
Part 2: Why FeNO first? Spotlight on testing & special cases
In Part 1, we explored the redefined approach to asthma diagnosis under the new NICE/BTS/SIGN guidelines. In Part 2, we dive deeper into the role of Fractional exhaled Nitric Oxide (FeNO) testing, looking at why it is now a frontline diagnostic tool and how it fits into broader asthma care, especially for children and those with occupational risks.
Why is FeNO now highlighted in the new guidelines?
FeNO has always been included in the guidelines and was central to the previous National Institute for Health and Care Excellence (NICE) guidelines for asthma care and management; however, the British Thoracic Society (BTS) and the Scottish Intercollegiate Guidelines Network (SIGN) previously only recommended FeNO to prove an asthma diagnosis. Now, all three have come together and recommended a FeNO test as a first-line diagnostic test for asthma.
Nitric Oxide (NO) is a gas we breathe out all the time; it is a normal part of the respiratory process. When a person has eosinophilic inflammation, more NO is produced, which results in a higher FeNO reading.
Occupational asthma
There is no new update to the guidelines on occupational asthma; the guidelines refer you to the BTS clinical statement for occupational asthma. It does state that if a patient has adult-onset asthma or poorly controlled established asthma, you should check if the symptoms are work-related, by asking the following questions:
Are your symptoms the same, better or worse on days away from work?
Are your symptoms the same, better or worse when on holiday or longer than usual breaks from work?
If symptoms worsen at work and occupational asthma is suspected, the patient should be referred to a specialist.
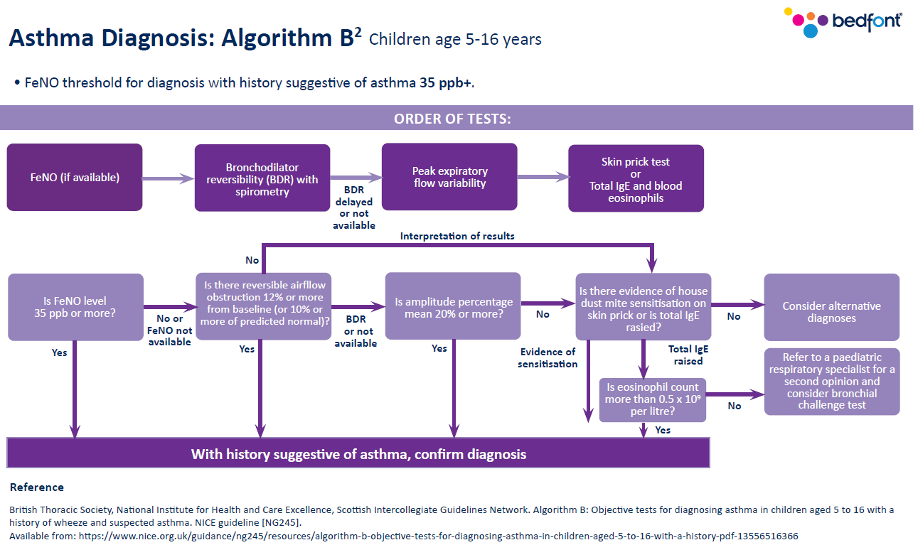
Asthma diagnosis in children (Aged 5-16)
As with adults, once a clear history and physical examination has taken place and asthma is suspected, you can move on to carrying out tests.
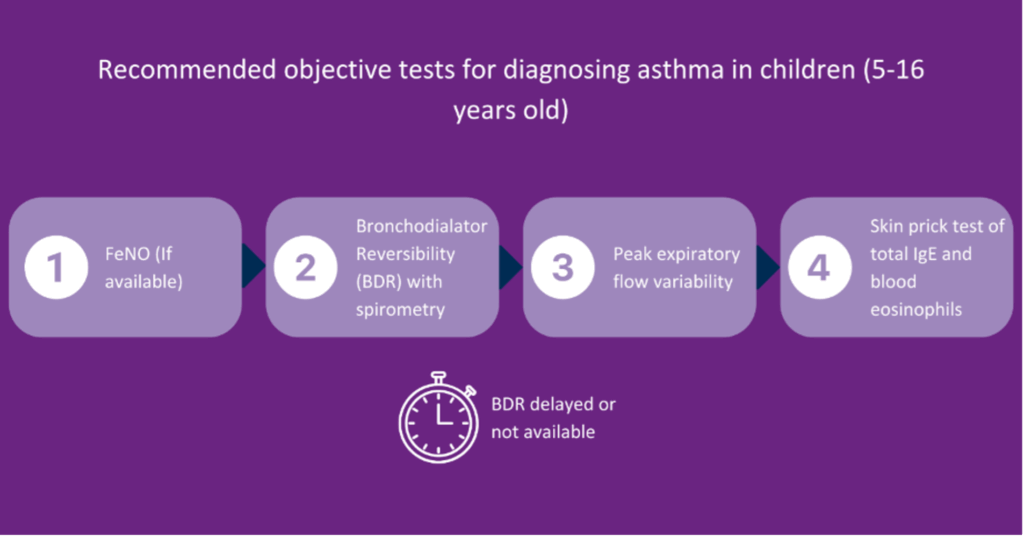
The first and only recommended test for children is a FeNO test. This means that a FeNO device should be available in primary care.
If the FeNO result does not support an asthma diagnosis, you should move on to bronchodilator reversibility (BDR) with spirometry. However, children on the younger side of the age bracket may find this test very challenging.
If this is the case, the guidelines recommend you move on to a peak flow diary.
A skin prick test is recommended if the peak flow diary results do not suggest asthma. Unfortunately, skin prick testing is not widely available, so this may not be possible.
Blood eosinophils are recommended last due to the invasiveness of the test.
How can you incorporate FeNO testing?
In some Primary Care Networks (PCNs), nursing teams have short slots available daily to perform FeNO tests on the day of presentation. This means the entire nursing team is trained to perform and correctly code a FeNO test and result. This approach, however, is not always possible in some settings, so some will ensure all clinicians are appropriately trained. This means that patients can receive instant results, start treatment immediately in the same appointment, and be referred to the asthma specialist for a follow-up.
Children under 5 years old
Previously, healthcare professionals (HCPs) were told not to diagnose asthma in children under 5 years old; it was recommended that they wait until they were 5 years old to make a diagnosis.
The new guidelines recognise that diagnosing this age group is challenging, as young children do not have the breath control required to take a test.
The recommendations in the new NICE/BTS/SIGN guidelines are:
If you suspect asthma, use your clinical judgement to treat and review regularly.
Once the patient reaches 5 years old, attempt to test for asthma. However, it is unclear whether treatment should stop before the test.
If the test is unsuccessful, continue treatment with regular reviews.
Re-attempt the tests every 6-12 months.
If the patient is not responding to treatment, refer them to a specialist, as it may not be asthma.
The guideline also recommends that any preschool child admitted to the hospital or had two or more emergency care visits because of respiratory issues in 12 months be referred to a specialist.
What’s next?
With a clearer understanding of FeNO testing and its applications, we will now focus on how these new guidelines reshape asthma treatment and long-term management. In Part 3, we will cover therapy options across age groups, medication strategies, and key recommendations for improving asthma control.
To keep up to date with our upcoming webinars, please follow us on social media or visit our website here.
Part 1: Understanding the changes – Asthma diagnosis & first steps in the new guidelines
In light of the recent update to the National Institute of Care Excellence (NICE) guidelines for asthma care and management, Bedfont® Scientific Limited sponsored an informative webinar by Intermedical (UK) Limited. Seasoned respiratory nurse Carol Stonham MBE led the session, where she discussed the changes to the guidelines in detail and why Fractional exhaled Nitric Oxide (FeNO) testing is vital to the asthma pathway.
In this first part of our three-part series covering this insightful webinar, we focus on the foundations: patient-centred care, changes in diagnostic criteria, and the importance of the structured clinical assessment.
Carol Stonham MBE, has been a registered nurse since 1986, transitioning from acute hospital settings to primary care by 1990. She serves at the Gloucestershire ICB and leads the Respiratory Clinical Programme Group, as well as co-leading the NHSE South West Respiratory Network. Carol is also a member of the Bedfont® Medical Advisory Board.
Intermedical (UK) Limited are a leading specialist provider of medical diagnostic and therapy equipment in the UK’s cardio-respiratory healthcare sector. Trusted in respiratory health since 1997, they are the exclusive distributor of the Bedfont® NObreath® FeNO device in the UK.
Usually, guideline updates involve adjustments to recommendations here and there, but this update represents a seismic shift in how asthma is diagnosed and managed. This blog will examine what the guidelines tell us and where FeNO fits in.
The first recommendation, which healthcare professionals (HCPs) must be aware of and follow, is that healthcare should be patient-centred. Patients should be given enough time and information to make informed decisions about their care. Unfortunately, this can be tricky if the areas in which the HCPs work have a restrictive formulary.
How is asthma diagnosed?
Firstly, as a HCP, you should take a good and clear history to ensure asthma is suspected before you test for it. It is easy to see a cough or a wheeze, but this is not how a diagnosis should be made.
The recommendation has gone from HCP-reported wheeze to just “reported wheeze”. This is something to be cautious about, as the patient’s interpretation of a wheeze could be very different from what a HCP interprets as a wheeze.
Noisy breathing, cough, and chest tightness are the symptoms you could expect someone with asthma to have, but it is important to remember that they should vary. This means the symptoms are not the same every day; the variation could be the time of day or time of year, for example.
The patient should be able to identify triggers, such as “my symptoms are worse when I go from warm to cold”, etc.
You should ask about a family history of atopic disorders and be sure that the symptoms are not due to anything else. All other possibilities should be ruled out before you arrive at asthma.
Previously, the Quality and Outcomes Framework (QOF) said that more than one objective test is sufficient for an asthma diagnosis, and the British Thoracic Society (BTS) and the Scottish Intercollegiate Guidelines Network (SIGN) said you could diagnose asthma with no supportive tests.
The new joint guideline from NICE/BTS/SIGN brings clarity and consistency to asthma diagnosis, stating that a diagnosis can be made with a suggestive clinical history and just one supportive objective test, making the process easier for HCPS to follow.
As mentioned in the previous guideline, when an asthma diagnosis is made, it must be recorded how you came to that diagnosis. This is an important step, as if further down the line the patient is not responding to treatment, the HCP can go back to the diagnosis and see how the diagnosis was made to be sure it was correct.
What to do with patients who are presenting?
Typically, two groups of people present in primary care: those who come in looking and feeling perfectly well but say they have been wheezy and tight-chested at times, but feel perfectly fine today. Then, some come in and are experiencing symptoms at the time, and when you delve into the history, you find that it has been going on for a little while and that something has tipped them into an exacerbation.
The guidelines say that patients must be treated if they are acutely unwell at presentation. It may be unsafe to send them away without treatment while you wait for tests. If possible, carry out a test there and then, and if the patient is not well enough to take a test or the tests aren’t available, then it is recommended that you start treatment immediately and carry out the tests when possible. However, it is recognised that by doing this, the test results could return to normal due to the treatment.
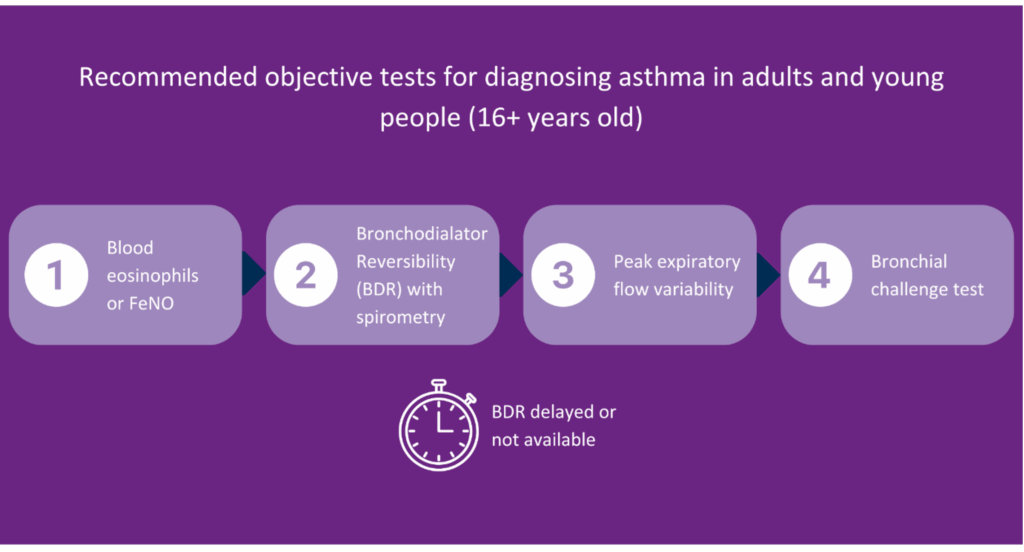
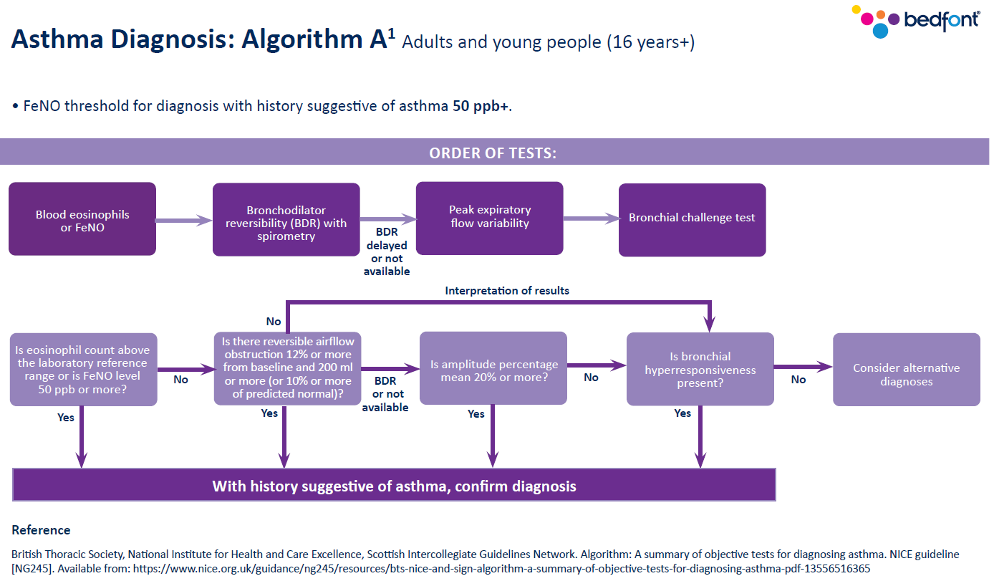
The guideline recommends the following tests for asthma diagnosis:
Blood eosinophils,
FeNO test,
Spirometry,
Peak flow with bronchodilator reversibility (BDR).
Ideally, you want to do the test there and then and choose the quickest and easiest option for the patient. Usually, tests such as spirometry and peak flow aren’t easy to do when the patient is unwell; therefore, a FeNO test would be the ideal option.
Patient examination
When examining a patient, you should look for the classic expiratory polyphonic wheeze. This is specifically seen in patients with asthma when they breathe out. However, patients presenting well that have reported being unwell may not have this wheeze, which should not rule out an asthma diagnosis, so testing should be conducted.
Test sequence
Once a clear history and a physical examination has taken place and asthma is suspected, you can move on to carrying out tests.
The first-line test for adults and young people over 16 is blood eosinophils or FeNO. While blood eosinophils may be considered appropriate for adults, a follow-up appointment to discuss the results would be required. It is possible to look up previous blood test results, but people, especially young people, do not often have regular blood tests, so this information may not be available. Unfortunately, primary care is usually short on time, so the quickest test option would be a FeNO test, if available. The test is quick and easy, non-invasive, and can be carried out within the same appointment.
If the blood eosinophils or FeNO result suggests asthma, you do not need to proceed any further with testing, as an asthma diagnosis can be made.
If these results do not suggest asthma, you should move on to BDR with spirometry. The guidelines recognise that spirometry isn’t as widely available as it should be, so if there is a delay in access to this test, you can move on to a peak flow diary.
If these further tests do not suggest asthma, you can move on to the bronchial challenge. However, this is a last resort test, not a test that should be carried out in primary care. A bronchial challenge test is high risk, and you should ensure easy access to resuscitation facilities.
We will look at the test sequence for children aged 5-16 in part 2.
What’s next?
Now that the groundwork for asthma diagnosis under the new guidelines has been laid out, it is time to look at the tools transforming how we confirm the diagnosis. In Part 2, we will explore why FeNO testing is taking centre stage and how it fits into asthma care across all age groups.
To keep up to date with our upcoming webinars, please follow us on social media or visit our website here.
The NObreath® device enhances access toFeNO diagnostics in Mexico.
Bedfont® Scientific Limited, a world leader in breath analysis with nearly 50 years of expertise in the medical breath analysis industry, has formed a strategic partnership with Aerosol Medical Systems to improve Fractional exhaled Nitric Oxide (FeNO) testing accessibility in Latin America. Aerosol Medical Systems is an established leader in the field of respiratory therapy, providing a comprehensive service to improve quality of life.
“We are committed to diagnosing and treating respiratory diseases and have completed, in collaboration with Bedfont®, the registration of the NObreath® device with the healthcare authorities in Mexico.” Comments Rodrigo León Molina, Director General and CEO at Aerosol Medical Systems. “The registration provides healthcare professionals with more accurate diagnostic tools and offers better treatment options for patients with asthma. This represents significant growth in the Mexican market, and will allow a larger number of tests to identify asthma early and better control the disease.”
In 2019, a report found that in Mexico, 1,655 people died from asthma1, highlighting the need for better asthma care across the region. The successful registration for the NObreath® FeNO device in Mexico is a vital step to improving the accessibility of innovative diagnostic and management tools for asthma care.
“Our mission has always been to provide cutting-edge medical devices at affordable prices to improve accessibility and healthcare standards worldwide.” Said Jason Smith, CEO at Bedfont®. “By collaborating with Aerosol Medical Systems, we’re helping clinicians across Mexico deliver faster, more personalised asthma care, empowering patients to live healthier lives.”
Working on a foundation of shared values, including providing exceptional service, this partnership aims to improve asthma care in Mexico by ensuring that those living with this respiratory condition have access to instant, non-invasive, and simple breath testing to aid diagnosis and management.
To learn more about the NObreath®, visit the website here.
References
1.Lopez-Bago A, Lascurain R, Hernandez-Carreño PE, Gallardo-Vera F, Argueta-Donohue J, Jimenez-Trejo F, et al. Sex, Age, and Regional Disparities in the Burden of Asthma in Mexico from 1990 to 2019: A Secondary Analysis of the Global Burden of Disease Study 2019. Sustainability [Internet]. 2023 Aug 20 [cited 2025 Oct 14];15(16):12599–9. Available from: https://www.mdpi.com/2071-1050/15/16/12599?